Ageing & Complex Medicine (Astley Ward) — Deprescribing in frailty
Project completed as part of Wrightington, Wigan and Leigh (WWL) Green Team Competition 2025.
Team members:
- Ðula Alićehajić-Bečić, Consultant Pharmacist Frailty
- Martin Farrier, Director of Digital Medicine, Chief Clinical Information Officer, Consultant Paediatrician
- Samuel Farrier, Pharmacist
- Donna Hewitt, Astley ward Manager
- Emily George and Alisha Maini, Polypharmacy analysis
Setting: Inpatient - Frailty Ward
Issue
Medicines contribute approximately 20% of NHS emissions, with a significant portion embedded in the pharmaceutical supply chain. Frail patients, who make up a large proportion of inpatient care, are particularly vulnerable to harm from inappropriate polypharmacy. Many long-term medications offer marginal benefit and may pose greater risks in this population, such as postural hypotension and falls. Despite this, deprescribing is rarely undertaken proactively and often only occurs after harm has already occurred.
Additionally, there is no formal system for assessing and reusing unused medications supplied to wards, leading to avoidable waste and environmental impact.
Intervention
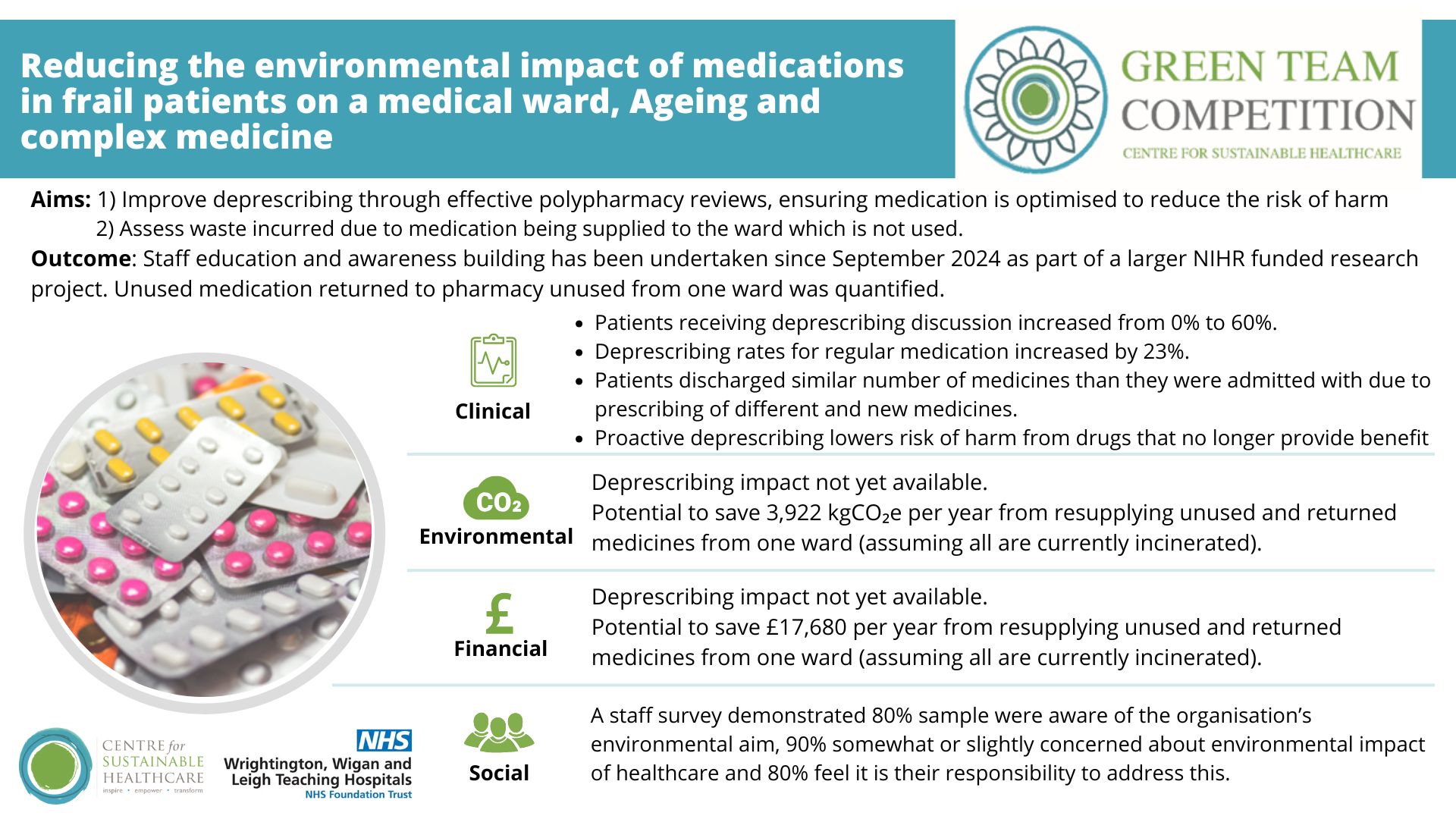
Aims 1) Improve deprescribing through effective polypharmacy reviews, ensuring medication is optimised to reduce the risk of harm
The ward became an active site for the NIHR-funded CHARMeR study in November 2024, which encouraged proactive deprescribing. Educational workshops were delivered to rotating doctors, consultants, and pharmacists, focusing on evidence-based deprescribing, barriers to implementation, and patient attitudes. A checklist was added to ward round notes to prompt deprescribing discussions.
Aim 2) Assess waste incurred due to medication being supplied to the ward which is not used.
Using the Clinical Informatics system, admission and discharge medication data were analysed for 20 patients in September 2024 (pre-intervention) and June 2025 (post-intervention). Staff were also asked to collect unused medications over one week for analysis of cost and carbon impact. A sustainability questionnaire was distributed to assess staff engagement.
Outcome:
Clinical
- Patients receiving deprescribing discussion increased from 0% to 60%.
- Deprescribing rates for regular medication increased by 23%.
- Patients discharged similar number of medicines than they were admitted with due to prescribing of different and new medicines.
- Proactive deprescribing lowers risk of harm from drugs that no longer provide benefit
Environmental and financial impact
- Aim 1: An increase in deprescribing rates was offset by a rise in newly prescribed medications, resulting in a similar overall medication numbers between admission and discharge. This was due to new clinical needs and substitution within drug classes, making it difficult to determine the true deprescribing impact. Further monitoring is needed to distinguish genuine deprescribing from medication switching.
- Aim 2: Potential to save £17,680 and 3,922 kgCO₂e per year from resupplying unused and returned medicines from one ward (assuming all are currently incinerated).
Social
- A staff survey demonstrated 80% sample were aware of the organisation’s environmental aim, 90% somewhat or slightly concerned about environmental impact of healthcare and 80% feel it is their responsibility to address this.
Key learning point
The project demonstrated that successful deprescribing in frail patients is supported through team-wide agreement that the issue is important and suitable to address. Staff engagement was critical, with education and ward round checklists helping embed deprescribing into routine practice. A systematic and coordinated approach, including data analysis, structured education, and workflow redesign, enabled the team to move from ad hoc reviews to a consistent, proactive process. Sustainability goals can be effectively integrated into clinical care when staff understand the problem, feel empowered to act, and are supported by clear systems.
Please log in or sign up to comment.